Quick Takeaway
The Quick Takeaway
- Body size is usually measured by Body Mass Index[1] (BMI) with BMI’s between 18.5 and 25 considered healthy, BMI’s between 25 and 30 defined as overweight and BMIs above 30 defined as obese.
- The relationship between body size and mortality and morbidity is investigated in epidemiological studies. These show that overweight and obesity are associated with increased risk of early death and a range of chronic diseases including, cardiovascular disease, diabetes and cancer.
- It is acknowledged that losing weight is difficult and that many individuals that lose weight regain it, leading to periods of weight cycling and an upward trajectory in weight over time.
- Some practitioners in the field argue against a focus on weight to promote health and recommend instead that individuals are encouraged to adopt healthy lifestyle behaviours. This is the Health at Every Size or HAES approach.
- Observational and longitudinal studies both demonstrate the benefits of adopting healthy lifestyle behaviours on mortality and morbidity. Typically, the lifestyle behaviours that are studied are not smoking, eating a healthy diet, being physically active and no more than moderate alcohol intake.
- Further examination of the data shows that whilst healthy lifestyle behaviours are important for a long and healthy life, weight also plays a role. In populations stratified by weight, all with healthy lifestyles, the groups with a healthy BMI have better health outcomes than the groups that are overweight or obese.
- Nevertheless, healthy lifestyle behaviours seem to be the most important factor for health; overweight and obese individuals with healthy lifestyle behaviours have better health outcomes than normal weight individuals with poor lifestyle behaviours.
- The qualification here is that the data show that being obese and healthy is a temporary state and that people transition from being metabolically healthy and obese, to being metabolically unhealthy and obese. It’s possible that some research that identifies an obese but fit group may not have sufficient length of follow-up.
- All this adds up to the best advice for a long and healthy life being the adoption of healthy lifestyles and maintaining a healthy weight, but this ducks the problem of how to achieve and maintain weight loss.
- The latest research suggests focusing on adiposity, particularly abdominal adiposity as a chronic disease requiring treatment and moving away from a focus on BMI.
[1] BMI is measured as weight in kilograms divided by height in metres squared and is formally expressed in Kg per meter squared Kg/m².
The Full Deal
Introduction
Body size is usually measured by Body Mass Index[1] (BMI) with BMI’s between 18.5 and 25 considered healthy, BMI’s between 25 and 30 defined as overweight and BMIs above 30 defined as obese. Waist circumference is also used to measure body size and it is used as a measure of abdominal adiposity. For women a waist circumference of less than 80cm is considered to be low risk, whereas 80—88cm is considered high risk and more than 88cm is very high risk. For men, low risk is less than 94cm, high risk is 94-102 cm and very high risk above 102cm. People in the overweight and obese categories, or in the high-risk groups, are encouraged to lose weight to improve their health outcomes. But is it that simple? Is it possible to be healthy with a larger body size, and the other side of the same coin, does a “healthy weight” always mean good health?
At first glance the evidence supporting the adverse relationship between BMI and life expectancy and between BMI and the development of non-communicable diseases appears overwhelming. These data are presented in the next two sections. Nevertheless, this body of evidence has been challenged and an alternative view put forward based on the concept of Health at Every Size (HAES). According to HAES, healthy lifestyle behaviours are more important than body size. As with many considerations in the field of health, an examination of the evidence suggests that both arguments have merit. The balance of the evidence indicates that healthy lifestyles are the best path to a long and disease-free life, but that body size does play an important role. The research that supports this more nuanced view is presented below.
Life Expectancy and BMI
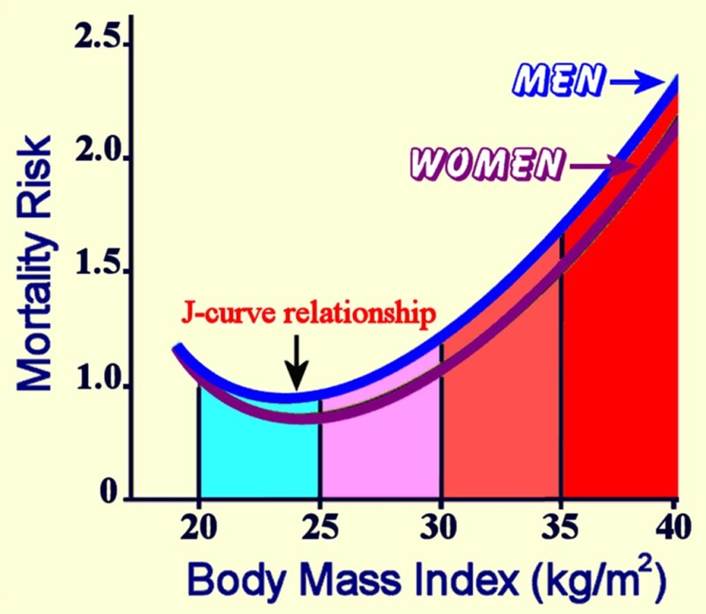
The relationship between body size and mortality is studied in populations, rather than in individuals. These studies are called epidemiological studies and involve large numbers of people followed for long periods of time. One such major study (Patel et al. 2014), which followed 900,000 people in the USA for 28 years found that mortality was increased in underweight, overweight and obese individuals compared to those with a healthy BMI (18.5-25). This type of relationship is described as a J shaped curve and is illustrated in the figure below[2]:
Interpreting the data from epidemiological studies can be complicated by confounding factors. Patel et al. (2014) controlled their data for smoking and pre-existing diseases both of which can appear to make lower BMIs healthy (because individuals that smoke or suffer from a chronic disease are typically thinner than other individuals in the population) and found that the relationship between BMI and mortality was strengthened.
The same J-curve relationship was reported by Bhaskaran et al. (2018) in an epidemiological study using data from primary care records in the UK and death registration data. The researchers had complete data on more than 3.5 million individuals, and they were able to separate out the population that had never smoked. They controlled for reverse causality resulting from chronic disease by excluding the first five years of follow-up. The results showed increased all-cause mortality in the low, overweight and obese groups compared to the healthy weight group. The same J-curve pattern was seen for men and women and for all age groups although the influence of BMI on mortality was strongest in the youngest group. The healthiest weight for individuals in the study, that had never smoked, was a BMI of 25.
The researchers (Bhaskaran et al. 2018) also looked at the relationship between BMI and the cause of death. They found that a healthy BMI of 21-25 reduced the chance of death from cancer, cardiovascular disease, respiratory disease, blood/endocrine diseases, liver cirrhosis, other digestive diseases, urogenital diseases and musculoskeletal disease.
The same relationship between BMI and life expectancy has been reported in research where data from multiple studies is combined. Berrington de Gonzalez et al. (2010), in a major review of the literature involving 1.46 million adults from around the world, found that a BMI in the range (22.5-24.9) was associated with the greatest longevity. In individuals that were physically active the optimal BMI range extended slightly upwards into the overweight range. A more recent review published in the Lancet (Berrigan et al. 2016) covering a population of 3.9 million participants found the strongest relationship between BMI and mortality for underweight and obese participants, but they also found an association between BMI and mortality in the overweight range.
Overall, the epidemiological evidence supports strongly a relationship between both obesity and overweight, and reduced life expectancy.
Morbidity and BMI
Research has also examined the relationship between BMI and the incidence of non-communicable diseases. The weight of the evidence demonstrates an association between increased BMI and many non-communicable diseases.
A recent study of 270,657 individuals in the US with linked health records examined the relationship between BMI and 16 health outcomes including cardiovascular disease, type 2 diabetes, chronic kidney disease, pulmonary embolism, deep vein thrombosis, liver disease, obstructive sleep apnoea, gastro-intestinal reflux disease and osteoarthritis. The authors found an association between obesity and all sixteen health conditions and a graded association such that the likelihood of having the disease increased with the level of obesity (Yao et al.2025).
This study is in line with the earlier findings of Dixon (2010) who reviewed the information available at that time. His paper includes an assessment of the relative risks of certain disease states in people with obesity. He concluded that people with obesity have five times the risk of a normal weight individual of developing type 2 diabetes and obstructive sleep apnoea, two to five times the risk of myocardial infarction and stroke and are one to two times the risk of developing breast, prostate and colorectal cancer. He argues that all these diseases and many more are linked to obesity because it can be demonstrated that they increase in frequency as BMI increases, there is a metabolic explanation for the relationship between obesity and the disease, and the likelihood of developing the disease decreases with weight loss.
Lassale et al (2017) looked at the relationship between body size and cardiovascular disease in a cohort of 17,640 patients, without a history of coronary heart disease or stroke, recruited from eight European countries and followed up for 12.2 years. They found an association between body size, as measured by both BMI and waist circumference, but stronger for the latter, and the risk of cardiovascular disease. They believe that the stronger association for waist circumference points to the role played by visceral adiposity as opposed to peripheral adiposity in the development of cardiovascular disease.
A review by Guh et al. (2009) of studies that looked at the effect of overweight and obesity on the likelihood of developing other diseases found that both overweight and obesity were associated with type 2 diabetes, cardiovascular disease, asthma, gall bladder disease, osteoarthritis and chronic back pain. The strongest association was seen between BMI and type 2 diabetes.
Despite the convincing data linking increased body size to both morbidity and mortality, the relationship has been challenged and described as an oversimplification. The next section examines the basis for this challenge.
HAES
The Health at Every Size (HAES) movement seeks to shift the health focus from body size and weight loss to the promotion of healthy lifestyle behaviours. The emphasis is firmly on healthy diet and physical activity and not on size. The proponents of this approach, for example Bacon and Aphramor (2011) cite data that show that many people seeking to lose weight go through cycles of weight loss and weight regain with an overall upwards weight trajectory. They argue that randomised controlled trials (RCTs) show benefits of an alternative HAES approach in terms of metabolic markers, eating behaviour or psychosocially by which they mean self-esteem, body image, depression and anxiety.
Supporters of the HAES approach challenge the data on the relationship between BMI and life expectancy, and BMI and morbidity from cardiovascular disease, diabetes and cancer, arguing that weight cycling has more serious adverse health consequences than BMI. They make a strong case that pursuing weight loss at the population level has not been beneficial for health, mainly because it is unsuccessful and therefore argue against body weight as a target for health interventions.
Bombak (2014) is an advocate for HAES who acknowledges the association between BMI and morbidity but argues, that for most conditions, causality has not been demonstrated. She states that ovarian cancer and osteoarthritis are the exceptions where causality has been demonstrated. For cardiometabolic health she recognises that several studies have linked poor cardiometabolic health to obesity, but she reframes the argument in terms of risk factors, and states that it is the number and magnitude of these risk factors that is higher in obese people than in normal weight people and that it is the risk factors that lead to the adverse health outcomes. In other words, she is saying that physical activity and diet influence health outcomes independently of BMI. She argues that as most individuals regain weight after a period of weight loss and because there are many biological mechanisms that encourage weight regain after weight loss, the focus should be on lifestyle factors, not body weight, to promote health.
Fat but Fit
To try and resolve this argument research has been carried out to ascertain whether it is possible to be obese, but metabolically healthy, based on a healthy lifestyle, and whether this is a transient or permanent state.
An important paper which seeks to answer this question is by Heath et al. (2022), a study based on UK Biobank data. The researchers considered four healthy lifestyle behaviours: never smoked, eating five or more portions of fruit and veg per day, being physically active and no more than moderate alcohol consumption. In a cohort of 339,902 participants with full health records the research team looked at all-cause mortality and cardiovascular disease risk across different groups divided by BMI. The also looked at metabolic complications, hypertension, diabetes and hyperlipidaemia. The follow up period was 11.4 years. As one might expect, there was a strong association between the adoption of healthy lifestyle behaviours and reduced incidence of cardiovascular disease, fatal cardiovascular disease and all-cause mortality. This association between healthy lifestyle behaviours and good health outcomes was maintained across all BMI groups, but the protection from adverse health outcomes provided by healthy lifestyle behaviours was reduced in the higher BMI groups. The overweight, obese and severely obese groups were at increased risk of cardiovascular disease, fatal cardiovascular disease and all-cause mortality compared with the normal weight group, and the risk increased with increased BMI.
The researchers (Heath et al. 2022) also looked at the impact of adopting healthy lifestyle behaviours within each BMI group. They found an association between healthy lifestyle behaviours and a lower risk of cardiovascular disease and all-cause mortality. This association was strong for smoking, but only weak for the other lifestyle behaviours studied. The presence of metabolic complications was associated with an increased risk of all poor outcomes, and this association was strongest in the higher BMI groups.
Overall, this large UK Biobank study (Heath et al. 2022), showed that adherence to healthy lifestyle behaviours offsets some, but not all the health risk associated with larger body size.
Appleton et al (2013) investigated the risk of developing metabolic diseases in a cohort of 3,743 Australian participants stratified by BMI. None of the participants were underweight. They found, over 5.5-10.3 years of follow up, that compared with metabolically healthy normal weight participants, those that were healthy and obese were more likely to develop metabolic risk factors and diabetes, but not cardiovascular disease over the follow-up period. Some of the obese participants maintained their metabolic health; these participants were younger than 40 and had lower waist circumference. The authors estimated that the metabolically healthy obese group represents 10-15% of the obese population and they commented that this group is likely to be unstable over time. They suggested that this switch from healthy to unhealthy occurs because of poor lifestyle behaviours.
Caleyachetty et al (2017) accessed 3.5 million patient records from primary care in the UK and linked these to hospital data. The researchers looked at the likelihood of developing cardiovascular disease in individuals that appeared to be metabolically healthy at the start of the study and whether this was influenced by BMI. They found that over five years of follow-up, individuals that were metabolically healthy at the start of the study, but were either obese or overweight, were at increased risk of developing cardiac disease and cerebrovascular disease compared to normal weight individuals. The risk of developing heart failure was increased in underweight, overweight and obese individuals.
Another study based on a specific UK population was published in 2008 (Khaw et al.). The participants were recruited in Norfolk and were mainly white and therefore not representative of the UK population as a whole. A survey of lifestyle behaviours was undertaken at the start of the study, BMI was measured, and fruit and vegetable intake was assessed by testing for vitamin C levels in the blood. Participants were followed for 11 years and health events were recorded. The researchers found that each of four adverse lifestyle behaviours namely smoking, more than moderate alcohol intake, low fruit and vegetable consumption and physical inactivity were associated with increased all-cause mortality. The mortality risk was higher in overweight and obese individuals compared to standard weight individuals for each healthy lifestyle behaviour. Nevertheless, in all weight groups, adopting healthy lifestyle behaviours reduced the mortality risk.
In a longitudinal study, Rassy et al. (2023) studied 438,583 participants from the UK Biobank. The mean age of the participants was 56.5, and 24.4% of the cohort were obese. Participants were followed for 12.8 years. The lifestyle factors investigated were diet, physical activity, alcohol consumption and smoking. Just over a third (34.3%) of the cohort developed at least one non-communicable disease over the follow-up period. The authors found that having healthy lifestyle behaviours protected the obese participants from developing non-communicable disease; the obese participants with four healthy lifestyle factors had a lower risk of developing cardiovascular disease, kidney failure, gout, sleep disorders and mood disorders compared with obese participants with no healthy lifestyle behaviours. Nevertheless, participants with obesity, compared to those without obesity, were at a higher risk of developing a non-communicable disease irrespective of lifestyle score. These data suggest that a healthy lifestyle cannot fully offset the adverse impact of obesity.
In seeking a relationship between lifestyle behaviours, BMI and health outcomes, length of follow up is important because healthy outcomes in response to high BMI and/or unhealthy behaviours accumulate over time. Veronese et al (2016) studied two cohorts of US based healthcare professionals with 32 years of follow up to examine the relationship between lifestyle behaviours and BMI on longevity. They recorded all-cause mortality and mortality from cancer and cardiovascular disease. For lifestyle behaviours they measured diet quality, physical activity, smoking and alcohol consumption, and recorded BMI. There were 114,136 participants and 30,013 deaths in the long follow-up period. The researchers found a clear relationship between BMI and mortality with the most healthy BMI being in the range 18.5-22.4. The adoption of healthy lifestyle behaviours mitigated the relationship between BMI and mortality such that both normal weight and obese groups improved their life expectancy if they followed healthy lifestyle behaviours. Their data imply that there is an advantage in adopting healthy lifestyle behaviours for all BMI groups.
In a study set up to separate out the health benefits of lifestyle behaviours and the impact on health of different body sizes, Matheson et al (2012) accessed data on US adults from the National Health and Nutrition Examination Survey. Data were collected between 1988 and 1994 and participants were followed up for an average of 14 years and 2 months. There were 11,761 participants and they were divided into three groups, normal weight (BMI 18.5-25), overweight (BMI over 25) and obese (BMI over 30). The authors took as a healthy baseline, being of normal weight and adopting four healthy lifestyle behaviours and the other groups were compared to this baseline. The healthy lifestyle behaviours studied were eating five or more portions of fruit and vegetables per day (an indicator of a healthy diet), undertaking regular physical activity, had no more than moderate alcohol intake and were non-smokers. In the overweight and obese groups, mortality decreased for each healthy lifestyle behaviour that was adopted. This implies that following a healthy lifestyle protects from the adverse health impact of being overweight or obese. Looking at the individual lifestyle behaviours, the researchers found that eating five or more portions of fruit and vegetables per day reduced mortality in the normal weight group and in the overweight group, but not in the obese group. Regular exercise was associated with decreased mortality in the normal weight and obese groups but failed to reach significance in the overweight group. The authors concluded that healthy lifestyle behaviours decrease mortality irrespective of baseline BMI implying that everyone needs to embrace a healthy lifestyle irrespective of BMI.
Metabolically healthy obesity?
Many other researchers have challenged the metabolically healthy obese concept. Zhou et al. (2021) followed 381,363 participants from the UK biobank. They defined metabolically healthy obesity as a BMI greater than 30 and having at least four out of six healthy metabolism criteria. The measured outcomes were the development of chronic diseases, cardiovascular disease, type 2 diabetes and respiratory disease. They found that people with metabolically healthy obesity had better outcomes than those who were obese with an adverse metabolic profile, but they had a higher risk of developing chronic diseases than metabolically healthy individuals living without obesity. The researchers also found that metabolically healthy obesity was a transient state with one third of the members of the group transitioning to metabolically unhealthy over the course of the study. The authors commented that metabolically healthy obese is a heterogenous group as some in this group did not go on to develop adverse health events. The authors were not able to predict which members of the metabolically healthy obese group would remain in this state.
Eckel et al (2016) conducted a systematic review and meta-analysis of papers looking at metabolically healthy obesity. They analysed data from 22 prospective studies and found that participants with metabolically healthy obesity were at increased risk of cardiovascular events compared with normal weight people, but that their risk was lower than both unhealthy normal weight people and unhealthy obese people.
Echouffo-Tcheugui et al. (2018) argue that their data, based on a cohort of 4,291 participants from the Framingham study[3], show that metabolically healthy but obese, is a temporary state and a “harbinger of future risk”. They divided the participants from their cohort into four groups: metabolically healthy/non-obese, metabolically healthy/obese (4% of the cohort), metabolically unhealthy/non-obese (31% of the cohort) and metabolically unhealthy/obese. In the follow up period they identified mortality, cardiovascular disease, type 2 diabetes and chronic kidney disease. They found a transition between the groups over time such that the four-year probability of moving from metabolically healthy obese to metabolically unhealthy obese was 43% in women and 46% in men. The metabolically healthy obese group had increased sub-clinical cardiovascular disease and coronary artery calcification compared to the normal weight metabolically healthy group, but the incidence of these signs was lower than in the metabolically unhealthy obese group. Over the 14 years of follow up, the metabolically healthy obese group had a higher risk of developing hypertension and diabetes compared to the metabolically healthy lean participants. The authors argue that when increased risk of disease is not reported in metabolically healthy obese participants, it is because the length of follow-up is insufficient for the adverse outcomes to be seen.
Thus, these large population based surveys demonstrate that healthy lifestyle behaviours protect people from mortality and morbidity even at BMIs that are in the overweight and obese range. Nevertheless, being overweight or obese are risk factors for mortality and morbidity.
Multimorbidity
Many individuals suffer from more than one health problem (multimorbidity). Kivimaki et al (2022) looked at the association between obesity and non-communicable diseases in multimorbid individuals drawn from two cohorts, one Finnish (14,657 participants) and one from the UK (UK Biobank, 499,357 individuals). These researchers looked at 78 predefined diseases. Most of the reported results are drawn from the Finnish cohort with supporting data from the UK cohort. They found that obesity was associated with 21 major diseases. Importantly they found that the risk of multi-morbidity was 12.4 times higher in obese individuals compared to normal weight individuals. Patients with obesity experienced multimorbidity at a much younger age than those with normal weight. The same pattern was seen in overweight but was much less pronounced. There was a dose response relationship between the degree of obesity and the likelihood of multi-morbidity. The risk of complex multimorbidity was greater in participants who developed obesity at a younger age (less than 50) compared with those who developed obesity later in life.
In this study the effect of obesity on mortality was much smaller than its effect on morbidity indicating that obesity decreases disease free survival more than overall survival. This means that obesity is a marker of a shorter healthy life expectancy.
What about people that are overweight but not obese?
Most of the research in this area has focused on comparing obese groups with normal weight groups. Where there is research on overweight people the results are more nuanced. The large UK Biobank study (Heath et al. 2022) for example found that in the overweight group with no metabolic complications and adopting healthy lifestyle behaviours there was an increased risk of cardiovascular disease, but not cardiovascular disease mortality or all-cause mortality compared to the normal weight group. The authors suggest that this finding may be due to medical management of cardiometabolic risk factors.
A systematic review and meta-analysis by Opio et al (2020) covering 23 studies and almost 4.5million participants found that metabolically healthy overweight and obese people were both at risk of cardiovascular disease compared to metabolically healthy normal weight people.
A study by Lin et al (2021) looked specifically at cancer risk. They studied 5,734 Taiwanese adults for an average follow-up of 12.7 years. They found that those classified as metabolically healthy but overweight or obese were at increased risk of developing cancer compared to the participants of normal weight.
The data indicate that there is a dose response type relationship with the adverse health effects of obesity more obvious than those of overweight but that being overweight, particularly with central adiposity is a health risk.
And people with a healthy BMI but abdominal adiposity?
A study that drew on survey data from 91 countries with 471,238 participants looked at the relationship between central adiposity with healthy BMI and health outcomes (Ahmed et al. 2025). The study found that 21.7% of the survey participants had a normal BMI but central adiposity as measured by waist circumference. In this normal BMI group, the researchers found a relationship between central adiposity and markers of poor metabolic health including hypertension, type 2 diabetes and blood cholesterol. They also found that a high waist circumference was associated with a poor diet, as measured by low consumption of fruit and vegetables and lack of physical activity. This study further supports the importance of lifestyle factors and not over relying on a single measure like BMI. Central adiposity is more difficult to measure but may be a more reliable health indicator.
Is there a lean and unhealthy group in the population
The research presented here shows clearly that it is possible to be of a healthy weight according to BMI but to be at risk of a range of non-communicable diseases. People may be in the lean but unhealthy group for two reasons. First, they may not have a healthy lifestyle, they may smoke, eat a poor diet, be physically inactive or overconsume alcohol, all of which put them at increased risk of non-communicable disease compared to people who are of healthy weight and follow a healthy lifestyle. Second, this group may contain individuals who are already suffering from a chronic disease or have a yet to be diagnosed chronic disease that is contributing to their low BMI.
Musculoskeletal Disease
Most of the work examining the relationship between body size and chronic disease focuses on metabolic diseases, cardiovascular disease and cancer. Body size plays a role in other common disease. Obesity is acknowledged to be a major risk factor for the development of osteoarthritis (Pottie et al. 2006). Increased body mass causes the joint cartilage to become overloaded, and this increases the risk of osteoarthritis particularly in the knee. The evidence indicates that the link is more than increased pressure on the joint because there is a positive association between obesity and osteoarthritis in non-weight bearing joints such as the hands. The explanation is believed to be arise from obesity causing dysregulation in lipid metabolic pathways which in turn influence the development of osteoarthritis (Pottie et al. 2006).
The American Association of Orthopaedic Surgeons (AAOS) has published information papers on obesity and musculoskeletal care (AAOS 2015; AAOS 2022). The 2022 Statement makes it clear that “Obesity negatively affects the orthopaedic management of nearly all musculoskeletal disease processes”. The report states that obese individuals are many times more likely to require total knee replacement than non-obese individuals and that the incidence of complications arising from surgery are higher in obese individuals. Similarly obese patients are more likely to suffer from back problems such as low back pain, sciatica and slipped disc and obese patients that undergo spinal surgery experience higher rates of complications.
Walsh et al (2018) argue that it is body fat and not body weight that mediates the relationship between obesity and musculoskeletal disease. Obesity is usually defined in terms of BMI, a measurement that depends on body weight but does not distinguish between fat and muscle. Walsh et al.’s (2018) review of the literature found a strong relationship between fat mass and pain at many different body sites. Proposed explanations for this finding include the increase in cytokines secreted by adipose tissue and sub-clinical inflammation
Weight Loss or Healthy Lifestyles?
If it is accepted that lifestyle factors are important and that weight loss is advisable in obese and overweight people but that most people find it difficult to lose weight and instead go through periods of weight cycling, what should be the public health approach?
Suarez et al. (2024) in a review of the literature examined the benefits of a HAES approach as an alternative to conventional weight loss strategies. The review covered the literature published between 2013 and 2023 and identified 20 papers. Eight of the papers showed that enhancement of overall wellbeing from a HAES approach had a positive effect on health outcomes irrespective of weight loss. Results from the studies showed mixed outcomes for the HAES approach on body weight although diet quality improved. Results on metabolic parameters were also mixed. Overall, people felt better and had healthier relationships with food. The best results were achieved when nutrition advice was combined with a physical activity programme. Long term, eating behaviour was less likely to change, but the psychological improvements were maintained. Most of the reviewed studies were of women participants so their generalisability to the whole population is not known. Most of the studies were short term so the long-term effectiveness of the HAES approach is not clear. It should also be noted that this review was conducted before the wide availability of GLP-1 agonist drugs for weight loss.
It will be important to look at this issue again when the long-term impact of GLP-1 agonists on mortality and morbidity has been studied.
What does this all mean
Most researchers conclude that public health management should focus on both lifestyle behaviours and weight management. That still leaves the problem that individuals find weight loss very difficult and many regain weight after losing it.
Current thinking is to consider obesity, or more accurately, adiposity as a chronic disease, as a health risk and a gateway to other chronic diseases. Thinking this way puts the emphasis om the degree and type of adiposity, not on BMI. Clinicians are encouraged to consider the full range of biomarkers and their likely effects on the body and not rely on BMI. Busetto et al (2024) used a modified Delphi[4] process to develop a consensus on the diagnosis, staging and management of obesity. They concluded that body fat, particularly abdominal fat is a more useful indicator of future disease than BMI. They acknowledged that obesity may be symptomatic but that it can progress to causing health impairments and to being a serious cause of ill health. The authors also drew attention to people in the overweight category, according to BMI, who have high amounts of abdominal fat who are at risk of the diseases associated with increased adiposity.
References
AAOS 2015 Position Statement 1184 The Impact of Obesity on Bone and Joint Health
AAOS 2022 Information Statement 1040 Obesity and Musculoskeletal Care
Ahmed KY, Aychiluhm SB, Thapa S, Tegegne TK, Ketema DB, Kassa ZY, Kibret GD, Duko B,
Shifti DM, Bore MG, Nezenega ZS, Bedaso A, Hailegebireal AH, Bizuayehu HM, Dadi AF, Beyene T, Shaikh MF, Hassen TA, Seid A, Astawesegn FH, Belachew SA, Leshargie CT, Berhe FT, Mondal UK, Little D, Hewa Marambage KA, Mahmood S, Ross AG. Cardiometabolic Outcomes Among Adults With Abdominal Obesity and Normal Body Mass Index. JAMA Netw Open. 2025 Oct 1;8(10):e2537942. doi: 10.1001/jamanetworkopen.2025.37942. PMID: 41105408; PMCID: PMC12534855.
Appleton SL, Seaborn CJ, Visvanathan R, Hill CL, Gill TK, Taylor AW, Adams RJ; North West Adelaide Health Study Team. Diabetes and cardiovascular disease outcomes in the metabolically healthy obese phenotype: a cohort study. Diabetes Care. 2013 Aug;36(8):2388-94. doi: 10.2337/dc12-1971. Epub 2013 Mar 14. PMID: 23491523; PMCID: PMC3714523.
Bacon L, Aphramor L. Weight science: evaluating the evidence for a paradigm shift. Nutr J. 2011 Jan 24;10:9. doi: 10.1186/1475-2891-10-9. Erratum in: Nutr J. 2011;10:69. PMID: 21261939; PMCID: PMC3041737.
Berrigan D, Troiano RP, Graubard BI. BMI and mortality: the limits of epidemiological evidence. Lancet. 2016 Aug 20;388(10046):734-6. doi: 10.1016/S0140-6736(16)30949-7. Epub 2016 Jul 13. PMID: 27423263; PMCID: PMC5508818.
Berrington de Gonzalez A, Hartge P, Cerhan JR, Flint AJ, Hannan L, MacInnis RJ, Moore SC, Tobias GS, Anton-Culver H, Freeman LB, Beeson WL, Clipp SL, English DR, Folsom AR, Freedman DM, Giles G, Hakansson N, Henderson KD, Hoffman-Bolton J, Hoppin JA, Koenig KL, Lee IM, Linet MS, Park Y, Pocobelli G, Schatzkin A, Sesso HD, Weiderpass E, Willcox BJ, Wolk A, Zeleniuch-Jacquotte A, Willett WC, Thun MJ. Body-mass index and mortality among 1.46 million white adults. N Engl J Med. 2010 Dec 2;363(23):2211-9. doi: 10.1056/NEJMoa1000367. Erratum in: N Engl J Med. 2011 Sep 1;365(9):869. PMID: 21121834; PMCID: PMC3066051.
Bhaskaran K, Dos-Santos-Silva I, Leon DA, Douglas IJ, Smeeth L. Association of BMI with overall and cause-specific mortality: a population-based cohort study of 3·6 million adults in the UK. Lancet Diabetes Endocrinol. 2018 Dec;6(12):944-953. doi: 10.1016/S2213-8587(18)30288-2. Epub 2018 Oct 30. PMID: 30389323; PMCID: PMC6249991.
Bombak A. Obesity, health at every size, and public health policy. Am J Public Health. 2014 Feb;104(2):e60-7. doi: 10.2105/AJPH.2013.301486. Epub 2013 Dec 12. PMID: 24328657; PMCID: PMC3935663.
Busetto L, Dicker D, Frühbeck G, Halford JCG, Sbraccia P, Yumuk V, Goossens GH. A new framework for the diagnosis, staging and management of obesity in adults. Nat Med. 2024 Sep;30(9):2395-2399. doi: 10.1038/s41591-024-03095-3. PMID: 38969880.
Caleyachetty R, Thomas GN, Toulis KA, Mohammed N, Gokhale KM, Balachandran K, Nirantharakumar K. Metabolically Healthy Obese and Incident Cardiovascular Disease Events Among 3.5 Million Men and Women. J Am Coll Cardiol. 2017 Sep 19;70(12):1429-1437. doi: 10.1016/j.jacc.2017.07.763. PMID: 28911506.
Dixon JB. The effect of obesity on health outcomes. Mol Cell Endocrinol. 2010 Mar 25;316(2):104-8. doi: 10.1016/j.mce.2009.07.008. Epub 2009 Jul 21. PMID: 19628019.
Echouffo-Tcheugui JB, Short MI, Xanthakis V, Field P, Sponholtz TR, Larson MG, Vasan RS. Natural History of Obesity Subphenotypes: Dynamic Changes Over Two Decades and Prognosis in the Framingham Heart Study. J Clin Endocrinol Metab. 2019 Mar 1;104(3):738-752. doi: 10.1210/jc.2018-01321. PMID: 30339231; PMCID: PMC6349002.
Eckel N, Meidtner K, Kalle-Uhlmann T, Stefan N, Schulze MB. Metabolically healthy obesity and cardiovascular events: A systematic review and meta-analysis. Eur J Prev Cardiol. 2016 Jun;23(9):956-66. doi: 10.1177/2047487315623884. Epub 2015 Dec 23. PMID: 26701871.
Guh DP, Zhang W, Bansback N, Amarsi Z, Birmingham CL, Anis AH. The incidence of co-morbidities related to obesity and overweight: a systematic review and meta-analysis. BMC Public Health. 2009 Mar 25;9:88. doi: 10.1186/1471-2458-9-88. PMID: 19320986; PMCID: PMC2667420.
Heath L, Jebb SA, Aveyard P, Piernas C. Obesity, metabolic risk and adherence to healthy lifestyle behaviours: prospective cohort study in the UK Biobank. BMC Med. 2022 Feb 15;20(1):65. doi: 10.1186/s12916-022-02236-0. PMID: 35164754; PMCID: PMC8845299.
Khaw KT, Wareham N, Bingham S, Welch A, Luben R, Day N. Combined impact of health behaviours and mortality in men and women: the EPIC-Norfolk prospective population study. PLoS Med. 2008 Jan 8;5(1):e12. doi: 10.1371/journal.pmed.0050012. Erratum in: PLoS Med. 2008 Mar 18;5(3):e70. PMID: 18184033; PMCID: PMC2174962.
Kivimäki M, Strandberg T, Pentti J, Nyberg ST, Frank P, Jokela M, Ervasti J, Suominen SB, Vahtera J, Sipilä PN, Lindbohm JV, Ferrie JE. Body-mass index and risk of obesity-related complex multimorbidity: an observational multicohort study. Lancet Diabetes Endocrinol. 2022 Apr;10(4):253-263. doi: 10.1016/S2213-8587(22)00033-X. Epub 2022 Mar 4. PMID: 35248171; PMCID: PMC8938400.
Lassale C, Tzoulaki I, Moons KGM, Sweeting M, Boer J, Johnson L, Huerta JM, Agnoli C, Freisling H, Weiderpass E, Wennberg P, van der A DL, Arriola L, Benetou V, Boeing H, Bonnet F, Colorado-Yohar SM, Engström G, Eriksen AK, Ferrari P, Grioni S, Johansson M, Kaaks R, Katsoulis M, Katzke V, Key TJ, Matullo G, Melander O, Molina-Portillo E, Moreno-Iribas C, Norberg M, Overvad K, Panico S, Quirós JR, Saieva C, Skeie G, Steffen A, Stepien M, Tjønneland A, Trichopoulou A, Tumino R, van der Schouw YT, Verschuren WMM, Langenberg C, Di Angelantonio E, Riboli E, Wareham NJ, Danesh J, Butterworth AS. Separate and combined associations of obesity and metabolic health with coronary heart disease: a pan-European case-cohort analysis. Eur Heart J. 2018 Feb 1;39(5):397-406. doi: 10.1093/eurheartj/ehx448. PMID: 29020414; PMCID: PMC6198928.
Lin CJ, Chang YC, Hsu HY, Tsai MC, Hsu LY, Hwang LC, Chien KL, Yeh TL. Metabolically healthy overweight/obesity and cancer risk: A representative cohort study in Taiwan. Obes Res Clin Pract. 2021 Nov-Dec;15(6):564-569. doi: 10.1016/j.orcp.2021.10.004. Epub 2021 Nov 12. PMID: 34782258.
Matheson EM, King DE, Everett CJ. Healthy lifestyle habits and mortality in overweight and obese individuals. J Am Board Fam Med. 2012 Jan-Feb;25(1):9-15. doi: 10.3122/jabfm.2012.01.110164. PMID: 22218619.
Opio, Jacob & Croker, Emma & Odongo, George & Attia, John & Wynne, Katie & Mcevoy, Mark. (2020). Metabolically healthy overweight/obesity are associated with increased risk of cardiovascular disease in adults, even in the absence of metabolic risk factors: A systematic review and meta‐analysis of prospective cohort studies. Obesity Reviews. 21. 10.1111/obr.13127.
Patel AV, Hildebrand JS, Gapstur SM. Body mass index and all-cause mortality in a large prospective cohort of white and black U.S. Adults. PLoS One. 2014 Oct 8;9(10):e109153. doi: 10.1371/journal.pone.0109153. PMID: 25295620; PMCID: PMC4189918.
Pottie P, Presle N, Terlain B, Netter P, Mainard D, Berenbaum F. Obesity and osteoarthritis: more complex than predicted! Ann Rheum Dis. 2006 Nov;65(11):1403-5. doi: 10.1136/ard.2006.061994. PMID: 17038451; PMCID: PMC1798356.
Rassy N, Van Straaten A, Carette C, Hamer M, Rives-Lange C, Czernichow S. Association of Healthy Lifestyle Factors and Obesity-Related Diseases in Adults in the UK. JAMA Netw Open. 2023 May 1;6(5):e2314741. doi: 10.1001/jamanetworkopen.2023.14741. PMID: 37234008; PMCID: PMC10220514.
Suárez R, Cucalon G, Herrera C, Montalvan M, Quiroz J, Moreno M, Sarmiento-Andrade Y, Cabañas-Alite L. Effects of health at every size based interventions on health-related outcomes and body mass, in a short and a long term. Front Nutr. 2024 Oct 8;11:1482854. doi: 10.3389/fnut.2024.1482854. PMID: 39439526; PMCID: PMC11493725.
Veronese N, Li Y, Manson JE, Willett WC, Fontana L, Hu FB. Combined associations of body weight and lifestyle factors with all cause and cause specific mortality in men and women: prospective cohort study. BMJ. 2016 Nov 24;355:i5855. doi: 10.1136/bmj.i5855. PMID: 27884868; PMCID: PMC5122318.
Walsh TP, Arnold JB, Evans AM, Yaxley A, Damarell RA, Shanahan EM. The association between body fat and musculoskeletal pain: a systematic review and meta-analysis. BMC Musculoskelet Disord. 2018 Jul 18;19(1):233. doi: 10.1186/s12891-018-2137-0. PMID: 30021590; PMCID: PMC6052598.
Yao et al, 2025. Association between Classi, II or III obesity and health outcomes. NEJM Evid 2025 4 (4).
Zhou Z, Macpherson J, Gray SR, Gill JMR, Welsh P, Celis-Morales C, Sattar N, Pell JP, Ho FK. Are people with metabolically healthy obesity really healthy? A prospective cohort study of 381,363 UK Biobank participants. Diabetologia. 2021 Sep;64(9):1963-1972. doi: 10.1007/s00125-021-05484-6. Epub 2021 Jun 10. PMID: 34109441; PMCID: PMC8382657.
[1] BMI is measured as weight in kilograms divided by height in metres squared and is formally expressed in Kg per meter squared Kg/m².
[2] Kyrou I, Randeva HS, Tsigos C, et al. Clinical Problems Caused by Obesity. [Updated 2018 Jan 11]. In: Feingold KR, Ahmed SF, Anawalt B, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000-. Available from: https://www.ncbi.nlm.nih.gov/sites/books/NBK278973/
[3] Long term, multi-generational cardiovascular study based on people living in Framingham, Massachusetts
[4] In a Delphi process, experts in a field are asked to comment on the acceptability of a series of statements. The statements are modified in response to feedback until consensus is reached.